Groin Pain and No Flexibility
Groin Pain and No Flexibility
(Dr. med. Andreas Krüger @polotimes.co.uk) Polodoc Medical Insight April 2018
A bad combination
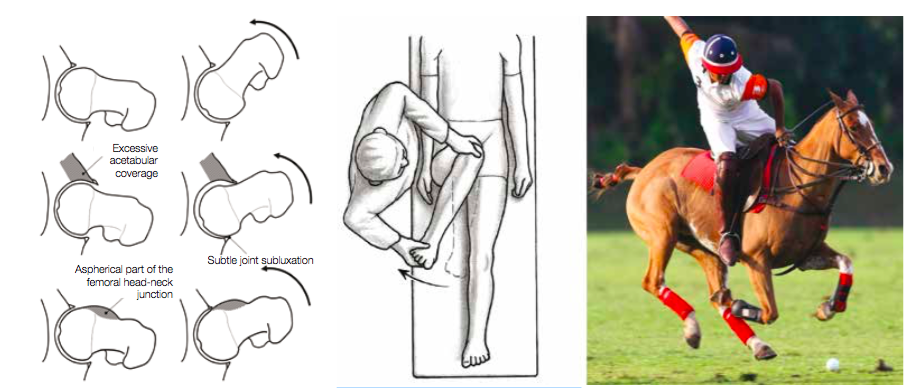
Flexibility to bend forward while standing in the stirrup and the freedom in the hip is key to reach out and win the ball in the one-to-one situation. Even while doing a regular polo swing and turning the upper part of your body, a relevant rotation in the hip is performed.
A reduced range of motion in the hip or a more relevant stiffness can lead to a pain problem limiting the performance of playing polo. The orthopaedic reason for this can be a mismatch between the ball and the socket of the hip, which is called femoral acetabular impingement (FAI).
How do I get FAI?
Some experts believe that significant athletic activity before skeletal maturity increases the risk of FAI, but no one truly knows. Sports with significant contact (i.e., football), with repetitive stress to the hip and male gender are associated with an increased likelihood of FAI.
Types of FAI
FAI generally occurs in two forms - Cam and Pincer. The Cam form describes the femoral head and neck relationship as aspherical or not perfectly round. This loss of roundness contributes to abnormal contact between the head and socket. The term Pincer (which comes from the French word meaning 'to pinch') describes the situation where the socket or acetabulum has too much coverage of the ball or femoral head. This over- coverage typically exists along the front-top rim of the socket (acetabulum) and results in the labral cartilage being 'pinched' between the rim of the socket and the anterior femoral head-neck junction. The Pincer form of the injury is typically secondary to 'retroversion', a turning back of the socket ('profunda'), a socket that is too deep ('protrusio'), or a situation where the femoral head extends into the pelvis. Most of the time, the Cam and Pincer forms exist together, otherwise known as 'mixed impingement'. FAI is associated with cartilage damage, labral tears, early hip arthritis, hyperlaxity, sports hernias and lower back pain. FAI is common in professional athletes, but also occurs in active individuals.

Prof. Dr. M. Tannast
Notes from Consulting Expert for Joint Preserving Hip Surgery Prof. Dr. M. Tannast of Bern University
1) Repetitive sports in adolescents can lead to an early onset alteration of the hip. 2) 50 percent of the cases are misdiagnosed as a 'sports hernia'. 3) The majority of problems can be solved with minor invasive surgery using arthroscopic methods.
Other reasons for groin pain
The most common cause of groin pain is a muscle, tendon or ligament strain, especially in athletes who play stop and go sports. Groin pain might occur immediately after an injury, or pain may come on gradually over a period of weeks or even months and will be worsened by continued use of the injured area. Less commonly, a bone injury or fracture, a hernia or even kidney stones might cause groin pain. Although testicle pain and groin pain are different, a testicle condition can sometimes cause pain that spreads to the groin area.
Groin pain commonly has its origins in the hip joints
The diagnosis of FAI
Patients will undergo a physical examination which will include:
The hip clinical examination should be
done with great care, because it provides the most reliable diagnostic information Physical findings will dictate further tests and necessary management.
Observation of a patient's sitting posture, gait, palpation of the hip, abductor strength testing, careful hip range-of- motion (ROM) assessment and specific provocative tests like the impingement test (rapid internal rotation of the leg in 90 degree flexion and adduction) should be performed.
Radiological examination: The investigation of FAI requires a combination of a roentgenographic examination and more sophisticated cross-sectional studies, such as magnetic resonance imaging (MRI) with performance of specific action.
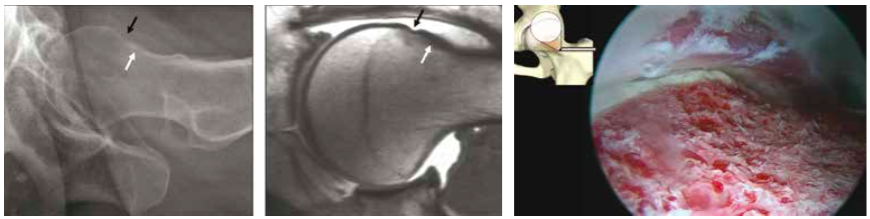
Cam type FAI in a 37-year-old woman and the joint after arthroscopic treatment
Treatment of FAI
Conservative treatment Activity restriction or cessation may alleviate symptoms in some patients. Athletes involved in repetitive hip flexion activities may experience significant relief of discomfort if they refrain from their sport. Although conservative measures are likely to be temporarily successful in some patients, those with a high activity level and athletic ambitions usually have low compliance. Conservative treatment may help and should be applied as a first-line treatment in symptomatic hips, especially those with mild and intermittent symptoms, before surgery is considered. Treatment may include activity restrictions, hydrotherapy, anti-inflammatory medicines and intra-articular injections. The severity of the clinical picture will dictate the eventual therapeutic methods used. Physical therapy, emphasising the improvement of passive hip ROM, or stretching, is counterproductive and should be avoided because it will irritate the hip and subsequently worsen the pain by sustaining and evolving articular surface damage.
Surgical treatment
Surgical treatment of femoroacetabular injury focuses on improving the clearance for hip motion and alleviation of femoral support against the acetabular rim. This includes the surgical resection of the injured area, by trimming the acetabular rim or the femoral head-neck offset either via a surgical hip dislocation or arthroscopically. Mid-term results from these procedures are promising.

Use of the Racewood Horse can provide a full analysis of the seat position and swing technique, here shown at reitsimulator.ch with an equine sport therapist
Diagnostics and possible adjustments of riding technique
With the use of the Racewood Horse, a full analysis of the seat position and swing technique off the field can be performed. The medical expert can detect and correct painful positions whilst in the saddle and performing the swing. Typical intra-game problems can be simulated and analysed. The focus here
is on posture with control of muscle power and use, as well as pelvic spine coordination and maybe, if indicated, adjustments of the equipment. A complete work up of the groin pain should be performed with a treatment plan consisting of all components of conservative and if needed of operative therapy should be discussed.
Checkbox
To reduce internal rotation and groin pain, please see an orthopaedic surgeon for a consultation.
Rule out additional or other causes of injury with a sports specialist.
A full assessment of riding techniques with the help of a simulator can help to minimise future mistakes.
For more information contact Andreas Krüger MD

Special thanks to J. Landry (photographer)